Professional guidance on the safe and secure handling of medicines
Published: 3 December 2018
This page has been archived
It still supports good pharmacy practice; however, you may find some outdated terminology or broken links.
Update (22 January 2024): Some of the content on this page is superseded by our new position statement and guidance.
This page was published when the organisation was the Royal Pharmaceutical Society.
Introduction
Medicines are used in all healthcare settings and the safe and secure handling of medicines is essential to ensure patient safety. The revision of the ‘Safe and Secure Handling of Medicines’ broadens the scope of the guidance to all healthcare settings and covers all pharmacists and other health professionals working whose role involves handling medicines.
The good practice guidance described in this online resource covers obtaining medicines, their transport, receipt, manufacture or manipulation and storage. It also includes information on the issuing of medicines, and their removal or disposal. Additional guidance is provided on the storage of medicines, the handling of controlled drugs and the safe and secure handling of medicines in theatres.
‘Safe and Secure Handling of Medicines’ is produced in line with the gold standard of NICE accreditation.
Scope
1.1 This guidance considers the processes associated with the handling of medicines. These include obtaining medicines, their transport, receipt, manufacture or manipulation, storage, issuing of medicines, and their removal or disposal.
1.2 The guidance applies to all medicines including: advanced therapy medicinal products*; biologicals*; blood products licensed as medicines, e.g. immunoglobulins (but not blood itself or non-licensed blood products); cytotoxics*; investigational medicinal products1 medical gases (but not industrial/laboratory gases, cryogenic agents, e.g. liquid nitrogen); radiopharmaceuticals*; and vaccines*.
*Separate guidance also applies to the handling of aseptically produced medicines.2
1.3 The guidance essentially deals with medicines however there may be situations where food supplements, borderline substances or medical devices which incorporate an active pharmaceutical ingredient (e.g. pre-filled sodium chloride 0.9% syringes) could also be considered within the same principles following appropriate risk assessment.
1.4 The clinical elements of the prescribing of medicines (such as choice of medicine, treatment duration, route of administration and monitoring of patients) are beyond the scope of this guidance.3
1.5 This guidance is relevant to all healthcare settings where medicines are handled and unless otherwise stated, it applies across all areas of practice. However, it may be the case that not every aspect of the guidance will be applicable in every setting.
1.6 Social care settings, e.g. care homes, are not specifically covered by this guidance. However, some of the principles are likely to apply and be of value to health and care professionals who work or advise on the safe use and storage of medicines in social care settings.
Further information on managing medicines in care homes can be found in the NICE social care guidelines.4,5
1.7 Medicines that are obtained and stored by patients in their own homes, are not directly within the scope of this guidance. However, some of the principles are likely to apply and be of value to health and care professionals who work or advise on the safe use and storage of medicines in peoples’ homes.
1.8 This document does not provide guidance for manufacturers or wholesalers who are subject to relevant good manufacturing or wholesale dealing practice guidance.
1.9 Application of this guidance is a multidisciplinary responsibility. All staff groups involved in the handling of medicines should be involved in developing organisational policies and procedures. Advice on interpretation of the guidance can be obtained from pharmacy professionals.
1.10 In addition to corporate and clinical governance responsibilities, healthcare professionals are personally responsible for putting patients and their safety first and for a commitment to ethics, values, principles and improvement. They are also responsible for practising within their own scope of practice and competence, including delegating where appropriate, and using their acquired knowledge, skills and judgement.6-11
1.11 This guidance provides the overarching principles needed to control the activities of handling medicines. Accordingly, it should also be used when developing policies and procedures and as a basis for the audit and quality improvement of the safe and secure handling of medicines. It is not intended to provide a detailed consideration of all possible circumstances in which medicines are used.
1.12 Specific guidance for the safe and secure handling of controlled drugs can be found in Appendix B – Controlled drugs.
1.13 This guidance complements the Royal Pharmaceutical Society(RPS) Professional Standards for Hospital Pharmacy Services, for the Reporting, Learning, Sharing, Taking Action, and Review of Incidents, Optimising Medicines for People in Secure Environments, and the RPS Professional Guidance for the Procurement and Supply of Specials.
1.14 Whilst references may relate to specific GB countries, in most cases they will have some relevance across the home countries.
Governance principles
2.1 The guidance in this document takes a quality management systems approach to the safe and secure handling of medicines.
2.2 The basic governance principles described in this document can be applied to all healthcare settings.
2.3 The four core governance principles that underpin the safe and secure handling of medicines are illustrated in Figure 1 below.
2.4 These governance principles are to be applied to each aspect of the safe and secure handling of medicines.

Principle 1: Establish assurance arrangements – ‘say what we do and why we do it’
2.5 The senior management/leadership team has overall accountability for the safe and secure handling of medicines in the organisation and supports this through corporate governance systems which are maintained and regularly reviewed.
2.6 The senior management/leadership team requires formal performance reporting mechanisms and is committed to promoting effective systems which take account of legislation and policy (national and organisational).
2.7 Such systems are supported by risk assessments, whilst at the same time considering patient and public safety within the healthcare setting.
2.8 The senior management/leadership team appoints a named individual (see Figure 2) who is responsible for setting the overall framework and policy standards for the safe and secure handling of medicines across the specific healthcare setting. The named individual is of sufficient seniority, knowledge and skills to provide leadership (relevant to the type of healthcare setting and with reference to the relevant legislation) and to promote awareness of the potential risks involved in the safe and secure handling of medicines and how they impact patient and public safety.
2.9 Where the named individual is not a pharmacy professional or member of the medicines optimisation team, e.g. Director of Nursing, Hospice Manager, Chief Nurse etc., advice is sought from a competent person with the relevant, knowledge, skills and experience when necessary.
2.10 Accountable individuals (see Figure 2) ensure that all organisation requirements are reflected in operational frameworks, procedures and plans. These are fit-for-purpose, and take into account all relevant legislation, national standards and guidance, as well as requirements from other stakeholders using the services of the organisation.
2.11 Accountable individuals use local context specific risk management policies to determine risks to medicines, patients and staff. Such assessments balance requirements for safety and security against the need to ensure that medicines are readily available to patients when needed.
2.12 The named individual ensures that accountable individuals are competent and supported in their role as it relates to the safe and secure handling of medicines.
2.13 Assessments are undertaken regularly (e.g. when new medicines or processes are introduced or changed), are documented where appropriate, and are used to inform risk mitigation, while also ensuring the management of remaining risks and ongoing improvement.
2.14 Accountable individuals ensure that policies and procedures such as standard operating procedures (SOPs) are approved by appropriate designated staff as defined in the organisation’s medicine policy or schedule of delegated authority.
2.15 Specific policies or procedures in line with relevant guidance and appropriate standards exist for each process that supports the safe and secure handling of medicines. These are dated and subject to routine update and review. Records of such reviews are maintained. Policies and procedures are available to any member of staff at the location where they are used.
Note: In smaller organisations, an individual may perform more than one of these roles, e.g. the named individual, may also be an accountable individual.

Principle 2: Ensure capacity and capability – ‘train people and ensure they have the necessary competencies and resources’
2.16 The organisation provides the required resources necessary to support the safe and secure handling of medicines and defines the following:
2.16.1 The people required, their knowledge, experience and skill mix.
2.16.2 The competencies, performance standards and responsibilities of these people.
2.16.3 The standard of the premises and equipment required.12,13
2.16.4 The environment including a suitable combination of human and physical factors.14
2.17 The roles and responsibilities of those involved in handling medicines are defined and recorded in policies.
2.18 Induction and ongoing training plans are in place and specify ongoing training requirements to maintain and update the knowledge, skills and experience of staff. Training records are maintained and updated.
2.19 Training competency standards are the same for all staff involved in the same or similar tasks in relation to the handling of medicines and competencies are demonstrated.
2.20 Performance and development reviews consider responsibilities around the safe and secure handling of medicines.
2.21 Persons authorised to handle medicines are accountable and comply with legal and registration frameworks, professional guidance and/or organisational or relevant national policy requirements.
2.22 Tasks are only delegated to persons who are legally entitled, authorised, appropriately trained and competent to handle medicines.
2.23 There are planned maintenance and replacement programmes for facilities and equipment to ensure continuing capability.
2.24 All materials, including equipment, containers, devices and packaging used for the safe and secure handling of medicines are fit for purpose.
Principle 3: Seek assurance – ‘do what we say and prove it’
2.25 Leadership within the organisation promotes an open and honest safety culture that supports the safe and secure handling of medicines.15,16 This is reinforced by proactive audit and review, and by reporting, sharing, learning and taking action on patient safety incidents.17
2.26 The quality assurance system for the safe and secure handling of medicines defines the organisational audit and monitoring processes which are used to check the standards of practice that are being delivered. A risk-based approach is taken to define the frequency of audit.
2.27 Routine audit is undertaken of all key processes and consequent remedial action, including escalation, is taken where necessary.
2.28 The process for identifying, resolving and learning from incidents and complaints is defined.
2.29 The named individual and accountable individuals embed a culture of assurance to ensure that policies, processes and plans are effectively implemented, and that all outputs are consistent with requirements specified in operational frameworks, policies and procedures.
Principle 4: Continually improve – ‘improve what we do’
2.30 The named individual is responsible for the oversight of the quality systems approach to the safe and secure handling of medicines delivered through the accountable individuals.
2.31 A culture of evaluation (both qualitative and quantitative) and learning and improvement is embedded throughout the healthcare setting; it is seen as everybody’s responsibility.18
2.32 Systems and processes are in place to ensure incidents are identified, recorded, investigated, reported and escalated where appropriate. Practice is reviewed, changed and shared to minimise recurrence, and any corrective or preventative action is monitored and reviewed.
2.33 Relevant incidents are fed into national and/or regional reporting schemes where they exist to support benchmarking, trending and learning on a wider basis.
2.34 Where identified, examples of good practice are shared and disseminated throughout the healthcare setting and with other organisations.
Framework
Introduction
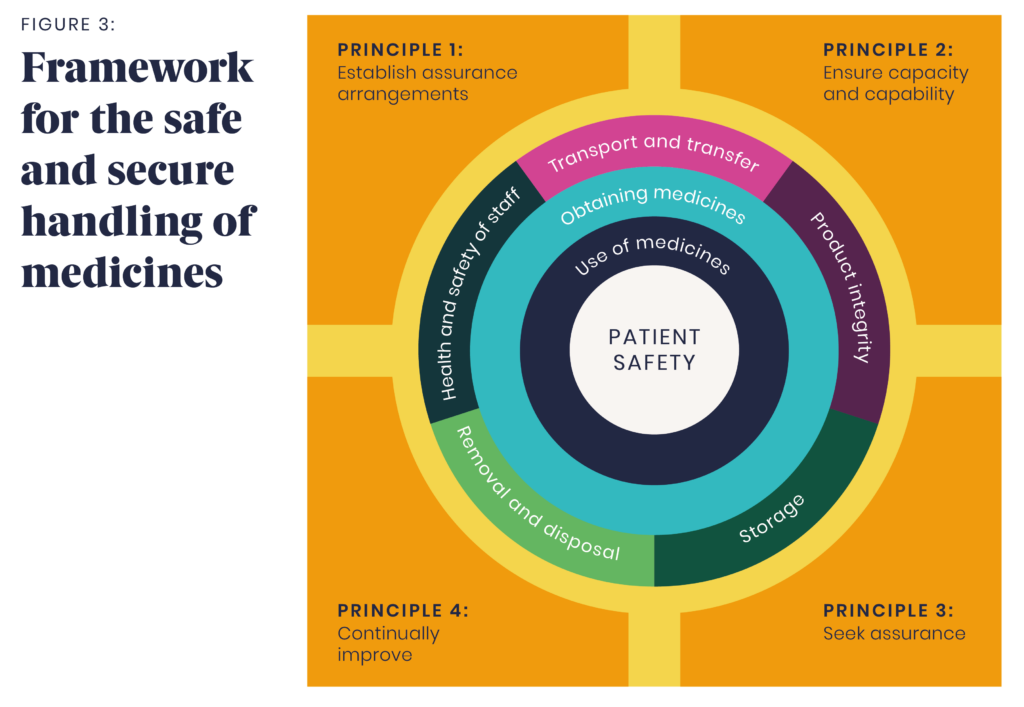
3.1 The framework for the safe and secure handling of medicines (see Figure 3) is intended to cover all potential activities that are associated with the handling of a medicine, from obtaining the medicine through to use and the disposal of any waste.
3.2 The four core principles that underpin the framework for the safe and secure handling of medicines are:
- Establish assurance arrangements,
- Ensure capacity and capability,
- Seek assurance, and
- Continually improve.
These principles are applied to processes that involve the handling of medicines throughout the framework (see Figure 3).
3.3 The framework needs to be applied to individual settings. Some aspects of the framework will always be present whilst others will only occur in specific settings/organisations or when certain medicines are used.
3.4 Appropriate links between all aspects of the medicines framework are established. Particular attention is taken to ensure safety and security of medicines when care, and medicines associated with that care, are transferred from one setting to another.19,20
3.5 All information necessary to assure continued safe use and security of those medicines is also securely transferred.
Obtaining medicines
3.6 Medicines are obtained from a reputable source and due diligence applied to ensure quality, their safe onward use and to minimise the risk of falsification.21
3.7 Organisational and legal requirements such as the Falsified Medicines Directive, Standing Financial Instructions22 and data protection are complied with.
3.8 Medicines are ordered/procured/requisitioned by legally entitled and authorised persons. See also section 3.19.
3.9 Issues such as availability, lead times and shelf life as well as the method of obtaining are considered.23
3.10 Policies and procedures to reduce risk are available for obtaining medicines, including those that cover specific categories of products such as investigational medicinal products and unlicensed medicines.24
Receipt of medicines
3.11 Where medicines are received from an external source, from the patient, or by transfer from one location to another within the organisation an audit trail exists.
3.12 Where medicines are being redistributed within an organisation this is done in accordance with organisational policies/procedures, e.g. dispensary or ward stock being moved to different sites within an organisation or to other pharmacies.
3.13 All medicines received are of the quantity and quality specified and are suitable for the purpose for which they are intended. Specific attention is applied to:
- confirm product identity and quantity
- ensure product integrity, e.g. that the cold chain and other storage requirements have been maintained where appropriate, and
- confirm compliance with any legal and/or organisational requirements.
3.14 The physical condition of medicines is protected by controlled storage, stock levels are monitored and records kept where appropriate. Policies and procedures consider environmental and security aspects of all storage locations, as well as the processes by which records of stock are maintained. See Appendix A: Storage of medicines, for further guidance.
3.15 Organisations have a policy in place and procedures for managing medicines (including items purchased ‘over-the-counter’, fridge items and controlled drugs) that patients bring with them into the healthcare setting, including that the medicines are assessed as fit for administration. These are drawn up in consultation with an appropriate pharmacy professional.
3.16 Policies and procedures consider current guidance on consent.25-34
3.17 Where medicines are brought into the healthcare setting by a patient one of the following processes is followed and all actions recorded:
3.17.1 The medicines are retained in the healthcare setting for the sole use of the patient during their stay. These are assessed and approved for use by appropriately trained staff following positive identification and assessment against defined quality criteria (including appropriate labelling). Responsibility and arrangements for security are covered in Appendix A: Storage of medicines.
3.17.2 The medicines are securely stored by the organisation until they are returned to the patient prior to or upon discharge unless a risk assessment indicates otherwise.
3.17.3 If no longer required, and the patient or the patient’s carer agrees, the medicines are disposed of or sent to a pharmacy or waste management company for destruction, as appropriate (see also section 3.28: ‘Removal and disposal of surplus and waste medicines’. If the patient requests, the medicines may be returned to the place where the patient lived via an identified adult. Responsibility for security is given to that adult. The patient and/or patient’s carer is advised if the medicines are not safe and/or appropriate for use.
3.18 A policy for self-administration in appropriate patients is in place. See also: RPS/RCN Professional Guidance on the Administration of Medicines.
Providing medicines to patients or a healthcare setting
3.19 Medicines are supplied to the place where they will be administered/used in response to formal requisitions. This can include patient labelled packs to supply under Patient Group Directions35 and medicines that will be supplied/administered under the Human Medicines Regulations 2012 exemptions (Schedules 17 and 19).36,37
Medicines are also dispensed directly to named patients in response to prescriptions, Patient Specific Directions38 or under the Human Medicines Regulations 2012 provision, e.g. emergency supply by a pharmacist.39
The different legal mechanisms that are used for the prescribing, supply and administration of medicines are given in Medicines Matters.40
3.20 Presentation and labelling of the medicine provided is consistent with legislation and is of a consistently acceptable standard.41-45
3.21 Automated and semi-automated systems are used to reduce risk and error where feasible and appropriate.
3.22 Where a care setting holds medicines as stock, a list of stock medicines and quantities to be held is determined by the relevant multidisciplinary team and is subject to regular review at agreed intervals.
Further reading
Health and Care Professions Council. Medicine entitlements. (Accessed 01/05/19)
Preparation of medicines in a pharmacy prior to administration
3.23 Where medicines are manufactured, prepared, manipulated or modified prior to administration these activities may be carried out in a suitably equipped pharmacy, or contracted out to NHS or non-NHS operated manufacturers under the appropriate licences.
3.24 Activities include:
- manufacturing of medicines from ingredients
- repackaging of medicines into small packs from bulk supply (including the use of multi-compartment compliance aids)
- over-labelling
- aseptic preparation of parenteral nutrition solutions, eye preparations, cytotoxics, biological and advanced therapy medicinal products
- reconstitution of injections, powders and oral suspensions
- addition of parenteral medicines to intravenous solutions, and the
- preparation of radiopharmaceuticals.46-48
Preparation of medicines outside of pharmacy prior to administration (near patient preparation)
3.25 Manipulation of medicines outside the pharmacy is minimised. Injectable medicines are presented as prefilled syringes or other ‘ready-to-administer’ preparations wherever possible, e.g. infusion bags.49-51 See also Appendix C – Operating theatres.
3.26 However, some form of preparation of the medicine may be necessary immediately prior to its administration. For example, the preparation of injections from vials or ampoules of dry powder and the preparation of mixtures. In these circumstances, measures are taken to prevent cross-contamination and to ensure infection prevention and control.
3.27 The activities associated with the preparation and labelling of injectable medicines are particularly high risk as these are fundamental to ensuring the correct dose of the correct medicine is administered to the intended patient. The injectables which present the highest level of overall safety risk include parenteral cytotoxic anticancer medicines, medicines subject to national alerts52,53 and any locally identified ‘high-risk’ injectable medicines. Their manipulation is as far as possible carried out under pharmaceutical supervision in a suitable controlled environment.54
Removal and disposal of surplus and waste medicines
3.28 National regulations and all legal requirements are met, e.g. Waste Management Regulations,55,56 Misuse of Drugs Regulations,57 and there is full compliance with organisational policy.
3.29 Waste medicines are appropriately segregated and stored securely, pending their disposal.
3.30 Medicines that patients bring in with them into the care setting, which are no longer required, are removed and/or disposed of with the agreement of the patient or the patient’s carer or in the interests of the patient/general safety.
3.31 Unused or unwanted stocks of medicines are returned to a pharmacy or a waste management company with appropriate security precautions.
3.32 Healthcare settings ensure that medicines which are out-of-date, damaged, no longer required or unsuitable for their intended use are disposed of or destroyed in a safe and secure manner in accordance with organisational policies/procedures.58
3.33 Organisational policies/procedures identify medicines at risk of diversion59 and/or illicit supply and such medicines are removed promptly and disposed of as soon as possible.
3.34 Records of destruction are kept where appropriate.
Transport and transfer
3.35 This covers the transport and transfer of medicines between sites within the same organisation as well as between one organisation and another and vehicles transporting medicines to treat patients (e.g. ambulances).
3.36 Organisational procedures are compliant with legal requirements and cover situations where staff transport medicines in the course of their duties.
3.37 Where third-party carriers (agents) are used, approved systems and controls are present, including the recording of collections and deliveries.
3.38 Transfers are managed under a system in which all orders and dispatches are authorised and recorded, and receipt of goods recorded. Staff engaged in the transport of medicines are identified, authorised and appropriately trained.
3.39 Procedures and equipment used in the transport of medicines are designed to ensure that the integrity and quality of the medicines are not compromised, e.g. to minimise temperature excursions within the cold chain (see also section 3.51 Product integrity).60
3.40 The security of medicines whilst being transported is risk assessed and steps are taken to ensure that risks are eliminated or minimised.
3.41 Arrangements for transport of controlled drugs61,62 medical gases63,64 and radiopharmaceuticals65 comply with any legal requirements and best practice guidance.
Storage
3.42 It is essential to ensure that planning and design of new premises incorporates appropriate facilities and sufficient capacity for the safe and secure storage of medicines.66,67
3.43 Policies and procedures are consistent with the general security arrangements within the organisation and relevant staff are involved from the design stage for new premises or equipment for storage.
3.44 From the time of receipt until use or removal, all medicines are kept secure and safeguarded from unauthorised access. Medicines are stored at a level of security appropriate to their proposed use at a level appropriate to their risk of diversion or risks in the local environment.
3.45 The level of security to be applied and the way in which this is achieved is balanced against the need to ensure timely access to medicines when they are required.
3.46 Medicines are stored at a level appropriate to the staff present at any time and access is restricted.
3.47 Procedures are in place to ensure that security is maintained in any storage area. These may be different in locations that are staffed continuously compared with those that are staffed intermittently even when the use of the medicine is the same in each area. Following risk assessment this may include remote monitoring and alarms.
3.48 At each stage where a medicine changes hands, there are clear policies/procedures explaining where the responsibility for security lies at that stage and the records required. The legal requirements related to the category of medicine are considered when developing these policies.
3.49 The security of medicines storage, including that in clinical areas, is checked regularly by a designated member of the multidisciplinary team and periodically independently scrutinised in accordance with organisational policy and procedures.
3.50 Pharmacy professionals apply this guidance in their own setting and also in care settings and clinical areas where they work, supporting other healthcare staff in these settings to apply the guidance where appropriate. Poor practice in relation to medicines storage, by any group of staff, is challenged, investigated and reported wherever and whenever it is identified.
Product integrity
3.51 All medicines, from whatever source, are subject to appropriate assessment of their fitness for use. Appropriate storage and environmental conditions are specified for all medicines.
3.52 Processes are in place to ensure that medicines are kept within the specified conditions to the point of use or disposal in all locations where they may be held or during transportation.
3.53 Ensure that any equipment or devices used for storage or administration (e.g. air tubes, IV lines and cannulae) do not threaten the integrity of the product.
3.54 Processes specify the required condition of a medicine at the time of use and the checks that are made to ensure it is used according to these conditions.
3.55 Sufficient data and information about the medicine is available to the staff and/or patient to enable them to identify the medicine and use it correctly.
3.56 The temperature of storage facilities is controlled and monitored. For items that require refrigeration or freezer conditions, the cold chain is maintained, and equipment used conforms to current guidance. See Appendix A: Storage of medicines.
3.57 When patients assume responsibility for their medicines under self-administration schemes, information and advice about maintaining the security and integrity of the medicine is given. See also RPS/RCN Professional Guidance on the Administration of Medicines.
3.58 Where conditions relating to product integrity have not been met or cannot be guaranteed any decision to use the medicine or not is fully risk assessed. Specific guidance is available for vaccines.68
3.59 The organisation has a policy for dealing with safety alerts and product recalls ensuring that affected products are quarantined as necessary (e.g. Drug Alerts issued by the Medicines Healthcare products Regulatory Agency).
Health and safety of staff
3.60 The risks associated with the processes of handling of any medicine are assessed for both staff and patients. This includes reference to legislative requirements, where necessary, such as Control of Substances Hazardous to Health (COSHH) and ionising radiation regulations.
3.61 Processes to minimise risks during transport, receipt, storage, preparation, and disposal of medicines are in place.
3.62 Equipment, devices, protective clothing and decontamination equipment (e.g. for cytotoxics) are available at the point of handling, as specified in the risk minimisation procedure.
3.63 Training is given to those handling any medicine and, where appropriate, competency checks are carried out at suitable intervals.
3.64 Policies/procedures cover actions to be taken in the event of unplanned incidents such as spillages of hazardous medicines; including recovery processes, record keeping and reporting.
Appendix A: Storage of medicines in health care settings — supplementary guidance
A1 Medicine storage meets national guidance and regulatory requirements. Governance arrangements are established using the four principles (see section 3.3) and audit trails are in place to underpin the storage of medicines.
A2 A risk management approach determines storage systems which reduce the risk of accidental access as well as unauthorised intentional access, whilst balancing the need for urgent or immediate access in clinical emergency situations.
A3 The storage of Schedule 2 controlled drugs (and where appropriate Schedule 3) meets the minimum requirements specified in legislation (where applicable) and prevents unauthorised access.69
A4 Cupboards and closed storage units in which medicines are stored and/or the rooms that accommodate these are lockable and locked when not being accessed.
A5 Medicines with differing routes/methods of administration, or which look alike/sound alike70 are stored separately or segregated to minimise selection errors. Risk assessments consider the latest national71,72 and local safety guidance to further segregate medicines at high risk of selection and/or administration error.
Examples include, but are not limited to:
- potassium chloride concentrate solutions
- organ perfusion fluids
- high strength opiates
- epidurals separately from intravenous infusions.
A6 Medical gases in cylinders are stored safely and securely73 to mitigate the following health and safety and diversion risks:
- cylinders are heavy and can cause severe injuries if mishandled
- cylinders contain compressed gas at high pressure and can cause severe injury or death if damage leads to sudden escape of gas
- oxygen supports combustion and increases the risk of fire
- other gases may cause suffocation if used inappropriately or may be subject to theft, diversion and abuse.
A6.1 Small size medical gas cylinders (e.g. size C, CD) are stored horizontally on shelves or in wall-mounted fittings. Larger cylinders are stored in a cage or secured to a fixed structure by a safety chain, at all times. When transported in vehicles such as ambulances, cylinders are secured appropriately so they cannot move in transit.74
A7 Areas where oxygen is stored or used display appropriate signage.75
A8 All medicines, including intravenous fluids and frequently used small volume injections in ampoules (such as dental cartridges, sodium chloride 0.9% and water for injection) are stored in their original packaging and not loose or decanted. Where this is not possible, risk assessments are undertaken and reviewed regularly.
A9 Non-medicines and chemicals such as disinfectants, diagnostic reagents (including those for urine testing), non-medicated dressings and dietary supplements, that may be accessed by people who would not otherwise have access to medicines are stored separately from medicines.
A10 Cupboards for the storage of medicines comply with the current British Standard 2881.
A10.1 Locks for cupboards (except patients’ medicine cabinets/lockers) comply with the current British Standard as a minimum. The current British Standard is BS 3621.
A11 Bulk flammable solutions are stored in lockable metal cupboards. A risk assessment is undertaken to determine whether a fire-resistant cabinet is required – this may not be required for small quantities in clinical areas.
A12 Access is controlled (by key or other means) to cupboards, trolleys and rooms where medicines are stored.
A12.1 Risk assessments are undertaken to determine the number of key copies and safe custody arrangements for these that are appropriate for the healthcare setting.
A12.2 Electronic locking systems that secure areas used to store medicines may use electronic keys, swipe cards or fingerprint and other technology that open the lock and lock immediately on closing the door. These systems allow cards or keys to be allocated to individual authorised persons, enabling audit of access to take place. Standard keypads where a number is shared with multiple users are not suitable for medicine cupboards.76 Where key pads are used on entry doors, the codes are changed at appropriate intervals subject to local risk assessment.
A13 Requirements for electronic medicines storage, issuing and locking systems are agreed locally. Issues such as access to power supply, IT connectivity and power failure back-up systems are considered where appropriate.
A14 Medicine trolleys are lockable and secured at an anchor point (i.e. a point at which trolleys can be secured to the floor or wall) when not in use. Alternatively, medicines trolleys may be stored securely in a locked room when not in use if access to the room is restricted to authorised persons.
Storage of patients’ own drugs
A15 All patients’ own medicines are stored securely.
A16 The level of security to be applied in the storage of patients’ own drugs, including controlled drugs, and the way in which this is achieved, is balanced against the need to ensure timely access to medicines when they are required.
A17 Where a personal locker/cabinet is used, a risk assessment determines the number of keys (or key cards/key fobs etc) available and responsibility for the master key.
Storage and access arrangements of medicines for clinical emergency77
A18 Storage arrangements allow for immediate access to critical medicines in the event of a clinical emergency, e.g. cardiac arrest or anaphylaxis. For further information on theatre settings see Appendix C: Operating theatres.
A19 These critical medicines are ready to administer preparations wherever possible and are held in containers, e.g. resuscitation boxes or crash carts/trolleys, which are tamper-evident, labelled appropriately, and clearly marked ‘for emergency use’. The locations of containers are clearly signposted.
A20 Unless a risk assessment has defined otherwise (e.g. in mental health units), containers are tamper-evident and are not held in locked cupboards or rooms, but at strategic and accessible sites.
A21 Policies and procedures are in place to ensure that boxes or crash carts/trolleys for clinical emergencies are maintained. This includes replacing used items as soon as possible, checking and replacing expired or damaged items, and defining who is responsible.
A22 Policies and procedures are in place to manage the risks of theft of and tampering with these medicines.
Temperature control
A23 Medicines are stored under conditions that assure their quality until they are used or administered including during transportation.
A24 A risk management approach is taken to determine suitable storage arrangements and monitoring requirements depending on individuals’ needs, the type and range of medicines stored, the length of time that medicines will be stored and local environmental factors including ambient room temperature.
A25 Any decision to store a medicine or use a medicine which has been stored outside the manufacturer’s recommended temperature range is fully risk assessed. Specific guidance is available for vaccines.78
A26 There is a policy in place, and procedures that outlines the actions to be taken if there is a temperature excursion outside the range specified for the medicines being stored and assurance that the procedure is followed.
A27 For items that require refrigeration or freezing, the equipment used is designed for the storage of medicines and conforms to current guidance.79-82
A28 The temperature of the refrigerator or freezer is monitored on each working day using a calibrated maximum-minimum thermometer or other approved monitoring device and a recording system is in place. This may be a fully automated system, or a manual reading which is recorded by the person who monitors the temperature.
A29 Staff reading the temperature are trained to ensure correct readings are recorded and that they understand how to reset thermometers where relevant. Where staff reading the temperature find that it is outside the accepted range they are aware of the actions to be taken to report and address this.
A30 Refrigerators and freezers are not overloaded to allow air circulation and medicines are not stored in contact with the sides or bottom of the refrigerator/freezer.
A31 Refrigerators and freezers are locked when not in use.
A32 Steps are taken to ensure that refrigerators and freezers are not accidently switched off.
A33 Refrigerators and freezers used for the storage of medicines are not used to store any other items.
Appendix B: Controlled Drugs — supplementary guidance
Legal framework
Controlled drugs (CDs) are defined and governed by the Misuse of Drugs Act (MDA) 1971 and associated Regulations – principally the Misuse of Drugs Regulations (MDR) 2001 which fall within the remit of the Home Office.
Persons using these guidelines should refer to the latest version of relevant legislation, including any amending regulations, as well as other associated guidelines, for up-to date information on the handling of CDs; for example:
- The Misuse of Drugs Act 1971 – the primary purpose of the MDA is to prevent misuse of CDs and makes it unlawful to possess or supply a CD unless an exception or exemption applies
- The Misuse of Drugs Regulations 2001 enable certain classes of persons to possess, produce, supply, prescribe or administer CDs in the practice of their professions. A list of the most commonly available CDs is published by the Home Office
- The Health Act 2006 introduced the concept of an ‘accountable officer’ and requires healthcare organisations, and those providing services to healthcare organisations, to have standard operating procedures in place for using and managing CDs
- The Controlled Drugs (Supervision of Management and Use) Regulations 2013 (England and Scotland) and The Controlled Drugs (Supervision of Management and Use) (Wales) Regulations 2008 (Wales) require all designated bodies to nominate or appoint a Controlled Drugs Accountable Officer (CDAO) to develop and implement systems for routinely monitoring the management and use of CDs and ensuring they are alerted to any risks, concerns and/or incidents
- The Misuse of Drugs (Safe Custody) Regulations 1973 control the storage of CDs
- The NICE guideline (NG46) Controlled drugs: safe use and management covers systems and processes for using and managing CDs safely in all care settings in England (except care homes).
Appendix B: Controlled Drugs – supplementary guidance
B1 Throughout this section and unless otherwise specified, ‘controlled drugs’ or ‘CDs’ refers to Schedule 2 CDs (and Schedule 1 CDs where appropriate). Risk assessments determine if other CD schedules are handled in the same way as Schedule 2 CDs within each healthcare setting.
B2 Where organisations are required to appoint a Controlled Drugs Accountable Officer (CDAO), the CDAO ensures the safe management and use of CDs (all Schedules) within the organisation, and ensures systems are in place for recording concerns and reporting incidents relating to the safe management or use of controlled drugs to, e.g. local intelligence networks.
B3 Where an organisation is not required to have a CDAO (e.g. general practice, dental clinic, community pharmacy) then a ‘Controlled Drugs lead’ is identified to perform this role within the organisation.
Information on the role of CDAO in England can be found on the Care Quality Commission website, in Wales on the Healthcare Inspectorate Wales website, and in Scotland on the Healthcare Improvement Scotland website.
B4 Arrangements are in place to detect unusual or poor clinical practice, to encourage good practice, and to detect and deter diversion. The arrangements do not interfere with the appropriate use of CDs and good clinical care.
B5 Controlled Drugs Accountable Officers (CDAOs)/CD leads ensure relevant individuals receive appropriate training and ongoing support in relation to CDs.
B6 A review, taking into consideration the framework for the safe and secure handling of medicines, evaluates the handling of CDs in the organisation and informs what policies and/or procedures are required.
B7 Up-to-date organisational policies and procedures (i.e. standard operating procedures [SOPs]) that comply with current legal framework are in place covering the management and use of CDs, such as (but not exclusively) the:
- security, including access to CDs
- ordering and receipt
- record-keeping, including audit requirements
- prescribing and clinical monitoring
- administration, including any witness requirements
- supply, including prompt access to ensure care is not compromised
- denaturing and disposal, including any witness requirements
- use and storage of patients’ own CDs
- transport (including transfer between care settings), including records
- investigation and reporting of concerns.
B8 Incidents involving CDs are reviewed with consideration of the root cause. Policies, procedures and associated learning are reviewed after a significant incident involving CDs, or when trends in incidents are identified. Any changes to policies and/or procedures are disseminated.
B9 The storage of Schedule 2 CDs (and Schedule 3 where appropriate) meets the minimum requirements specified in legislation (where applicable) and prevents unauthorised access.83
B9.1 Stored CDs are risk assessed and, where appropriate, separated for safety; e.g. high strength opiates84, patients’ own CDs and patient returns.
B10 CDs received, issued and denatured/disposed of by organisations are, where appropriate, recorded in a relevant CD register (paper or electronic).
B11 In larger premises, each area within the organisation that holds CD stocks (e.g. ward, department, theatre) keeps a record of CDs received, administered and returned or denatured/disposed of, in a CD record book (paper or electronic).
B12 The balance of all entries in the CD register/record book are checked and reconciled with the stock amounts in the cupboard.
B.12.1 The frequency of such checks is determined by risk assessment and ensures that discrepancies are identified promptly identified. In larger organisations operating on multiple sites, e.g. community pharmacy, dental practice or GP groups/chains, this may be determined at an organisational level.
B.12.2 Any discrepancies are investigated without delay and a local incident form completed. Unresolved discrepancies are reported to the CDAO/CD lead.
B13 Where part of an injectable CD is administered, the CD register/record book details the amount given and the amount denatured/disposed of.
B14 Individual doses of CDs which have been prepared but not administered are denatured and witnessed (in accordance with local risk assessment/procedures) and the reason documented.
B15 CDs are denatured prior to disposal in line with organisational policies and/or procedures.
Useful tools
Care Quality Commission. (2014). Controlled Drugs Self-Assessment Tool for Primary or Secondary Care Organisations.
Further reading
- Association of Anaesthetists of Great Britain and Ireland. (2006). Controlled Drugs in Perioperative Care.
- Association of Anaesthetists of Great Britain and Ireland. (2015). Position statement on administration of controlled drugs by anaesthetists for patient use.
- Royal Pharmaceutical Society. Medicines, Ethics and Practice – the Professional Guide for Pharmacists. (Accessed 31.01.18).
- Care Quality Commission. The safer management of controlled drugs annual report. (Accessed 20.08.18).
- Care Quality Commission. Nigel’s surgery 28: Management of controlled drugs. (Accessed 20.08.18).
- NHS Scotland and Controlled Drugs Accountable Officers Network Scotland. (2014). A guide to good practice in the management of controlled drugs in primary care – Scotland.
- National Institute for health and Care Excellence. (2016). NICE guideline (NG46) Controlled drugs: safe use and management.
- Specialist Pharmacy Services. (2016). How should dentists prescribe, store, order and dispose of controlled drugs?
Appendix C: Operating theatres — supplementary guidance
Includes some interventional areas such as radiology and cardiac catheterisation laboratories.
C1 As outlined in the core guidance, manipulation of medicines in clinical areas is minimised and medicines are presented as prefilled syringes or other ‘ready-to-administer’ preparations wherever possible, e.g. infusion bags.85-87
C2 All medicine-containing infusions and syringes are clearly labelled.88-90
C3 If medicines are drawn up and labelled in a theatre setting ideally this is done by the person who will administer them at the time of preparation.91,92
C3.1 Where this is not possible and when a practitioner requires that a medicine is drawn up on their behalf, e.g. when working in a sterile field, these medicines are:
C3.1.1 Checked with the requesting practitioner before they are opened
C3.1.2 Drawn up in the presence of the requesting practitioner – and checked (medicine, route of administration, diluent, dose, and expiry date) against the original container (e.g. vials) prior to administration.
C4 Adequate uncluttered surface space and appropriate trays, clean for each patient, are provided for drawing up, arranging and holding the syringes and drugs used in each procedure. Wherever possible this is standardised.
C5 Open systems (including gallipots and other types of open container such as moulded plastic procedure trays) are never used as containers for medicines – with the exception only of embolisation procedures involving embolic agents that need to be prepared openly.93-95
C6 Medicines for spinal, epidural or for nerve block injection are presented as prefilled syringes wherever possible and are clearly identifiable (e.g. as different coloured lines, bags and labels).90,96 Appropriate connectors are used for epidural, intrathecal and nerve block infusions.97
C7 Infusion pumps for epidural and/or nerve block infusions are permanently dedicated for a single purpose, and appropriately coloured and labelled.90 They have appropriate security and safety features, such as locks and pass codes.
C8 Medicines and fluids used in theatre settings are readily identifiable at all times during a procedure. Pre-labelled empty syringes and unlabelled or poorly labelled presentations are considered unsafe and immediately discarded.
C9 All local anaesthetic infusions are stored separately from intravenous infusion solutions and other safe segregation practices are used, e.g. paediatric IV fluids, epidural preparations,90 glucose98 and perfusion fluids.99
Useful tools
National Patient Safety Agency. (2007). Risk assessment tool for the preparation and administration of injectable medicines in clinical areas.
Further reading
- European Board of Anaesthesiology. (2016). Recommendations for Safe Medication Practice 2015.
- Royal College of Anaesthetists and the Association of Anaesthetists of Great Britain and Ireland. (2016). Storage of drugs in anaesthetic rooms.
Glossary
For the purposes of this guidance, the following glossary definitions apply:
| Term | Definition |
|---|---|
| Falsified Medicines Directive | Falsified medicines are often disguised as authentic medicines but may contain ingredients of bad or toxic quality, or in the wrong dosage. As they have not been properly checked for quality, safety and efficacy, as required by strict EU authorisation, they can pose a real risk to health. As falsified medicines become more sophisticated, the risk of them reaching patients in the EU increases. They represent a serious threat to global health and call for a comprehensive strategy both at European and international level. https://ec.europa.eu/health/human-use/falsified_medicines_en |
| Healthcare setting | Includes: ambulance trusts, community trusts, dental practices, dispensing doctor practices, GP practices, hospitals (NHS and private), mental health community services, pharmacies, private clinics (including physiotherapy and aesthetic), and secure environments |
| Patient | The term ‘patient’ refers to people receiving medicines and includes adults, children and young adults, service users, clients and in the in the case of maternity services, women. |
| Pharmacy professional | Registered professionals with the knowledge and skills in the safe and secure handling of medicines, namely pharmacists and pharmacy technicians. |
| Quality management system | A good system or a ‘quality system’ is a combination of sustainable structures, excellent leadership, right culture, good governance and processes, and a capable workforce all working together to enable continuous improvement and learning. www.pharmacyqs.com. See also ISO 9001: Quality Management. |
| Relevant staff | For example, named individual, local security risk management specialist, risk manager, security officer, local crime prevention officer. |
| Reputable source | For example, pharmacies (hospital or community), licensed wholesaler, manufacturer |
Acknowledgements
Task and finish group 2 (2018)
| Catherine Baldridge | Medicines Management Lead and Accountable Officer for Controlled Drugs, South Tyneside NHS Foundation Trust |
| Chris Bell | Standards Development Specialist, Nursing and Midwifery Council |
| Sarah Billington | Head of Medicines Optimisation, Care Quality Commission |
| Richard Cattell | Deputy Chief Pharmaceutical Officer, NHS Improvement |
| Alison Darbyshire | Quality Assurance Pharmacist, North West Regional Quality Assurance – NHS Specialist Pharmacy Service North |
| Steve Du Bois | Chief Pharmacist – Head of Medicines Management, Somerset Partnership NHS Foundation Trust |
| Tim Edwards | Consultant Paramedic, London Ambulance Service NHS Trust |
| Rachael Fallon | Deputy Director of Pharmacy and Head of Medicines Management, Manchester University Hospital NHS Foundation Trust |
| Katherine Gough | Head of Medicines Optimisation, Dorset Clinical Commissioning Group |
| Sarah Green | Chief Pharmacy Technician, Lancashire Care NHS Foundation Trust |
| William Harrop-Griffiths | Consultant Anaesthetist, Imperial College Healthcare NHS Trust – representing the Royal College of Anaesthetists |
| Karen Harrowing | Quality Systems and Pharmacy Consulting |
| Fran Husson | Patient/Lay Member; Honorary Research Officer, Imperial College London |
| Susanna Jacks | GP pharmacy representative, Royal College of General Practitioners |
| Yogini Jani | Consultant Pharmacist and EHRS Patient Safety Lead, University College London Hospitals NHS Foundation Trust |
| Victoria Lea | Regional Medicines Manager, Care Quality Commission |
| Carmel Lloyd | Head of Education and Learning, The Royal College of Midwives |
| Robert Lowe | Lead Quality Assurance Specialist Pharmacist – East of England, NHS Specialist Pharmacy Service |
| José Moss | Deputy Superintendent Pharmacist, Boots UK Limited |
| Richard Needle | Former Chief Pharmacist (now retired), Colchester Hospital NHS Foundation Trust |
| Janice Perkins | Chair, Community Pharmacy Patient Safety Group; Pharmacy Superintendent, Well |
| Wendy Preston | Head of Nursing Practice, Royal College of Nursing |
| Heather Randle | Professional Lead for Medicines Management and Non-Medical Prescribing, Royal College of Nursing |
| Tracy Rogers | Associate Director – Medicines Use and Safety, NHS Specialist Pharmacy Service |
| Tim Root | Specialist Pharmacist; Strategic Lead for Medicines, NHS Specialist Pharmacy Service; NHS London Procurement Partnership |
| Dipak Vaidya | Group Chief Pharmacist |
| Priti Ved | Deputy Chief Pharmacist (integrated Community/Child and Family Services), Coventry and Warwickshire Partnership Trust |
| Janice Watt | Lead Pharmacist Acute Services, NHS Greater Glasgow and Clyde |
| David Whittaker | Chair European Board of Anaesthesiology Patient Safety Committee |
Task and Finish Group 1 (2017)
| Tim Hanlon | Former Chief Pharmacist, Guys and St Thomas’ Hospitals NHS Foundation Trust |
| Karen Harrowing | Quality Systems and Pharmacy Consulting |
| Norman Lannigan | Former Head of Pharmacy and Prescribing Support Unit, NHS Greater Glasgow and Clyde |
| Richard Needle | Former Chief Pharmacist (now retired), Colchester Hospital NHS Foundation Trust |
| Tim Root | Specialist Pharmacist; Strategic Lead for Medicines, NHS Specialist Pharmacy Service; NHS London Procurement Partnership |
| Richard Seal | Regional Lead Pharmacist, NHS Improvement and NHS England |
Advisory Steering Group
| Hannah Abbott | President, College of Operating Department Practitioners |
| Jane Barnes | Pharmacy Manager, Nevill Hall Hospital – Aneurin Bevan University Health Board |
| Alan Borthwick | Emeritus Professor, School of Health Sciences, University of Southampton |
| Christine Buicke | Policy Manager, Standards and Ethics, General Medical Council |
| Nick Butler | Lead Pharmacist General Practice Education (Midlands), Centre for Pharmacy Postgraduate Education |
| Alan Clee | Advanced Pharmacist Controlled Drugs Governance, Controlled Drugs Accountable Officer Network Scotland |
| Sarah Dennison | National Controlled Drugs Manager, Care Quality Commission |
| Denise Farmer | Pharmaceutical Adviser Health and Justice, NHS England |
| Matthew Fitzpatrick | Consultant Podiatrist and Chair – Clinical Senate, The College of Podiatry |
| Katharina Floss | Critical Care, Theatres and Anaesthetics Directorate Pharmacist, Oxford University Hospitals NHS Foundation Trust |
| Sonia Gilmore | Lead Pharmacist – Pharmacy Governance, Nottingham University Hospitals NHS Trust |
| Matt Griffiths | Professor of Prescribing and Medicines Management, Birmingham City University; Nurse Practitioner in Urgent Care, The Royal United Hospital, Bath |
| Kashif Haque | Chief Pharmacist, East Cheshire NHS Trust |
| Peter Hawkes | Patient/Lay Member |
| David Heller | Chief Pharmacist, Surrey and Sussex Healthcare NHS Trust |
| Sarah Hudson | Lead Pharmacist, South West Yorkshire Partnership Trust |
| Malcolm Irons | Pharmacist, Specialist, Care Quality Commission |
| Mark Jackson | Director NW Regional QA Services, NHS Specialist Pharmacy Service |
| Sharon Jackson | NHS Pharmaceutical Quality Assurance Committee |
| Lynette James | All Wales Consultant Pharmacist – Acute Care and Medication Safety, Cardiff and Vale University Health Board |
| Sue Johnson | Professional Officer, Society and College of Radiographers |
| Monali Khachi | Medication Safety Officer, Lead Pharmacist – Risk, Compliance and Mental Health Rehabilitation Services, Central and North West London NHS Trust |
| Amanda Laird | Advanced Pharmacist Addictions, NHS Greater Glasgow and Clyde |
| Nigel Langford | Consultant Clinical Pharmacology and Acute Medicine, Royal College of Physicians |
| Nicola Lewis | Highly Specialist Pharmacist – Urgent Care, Barts Health NHS Trust |
| Janet Long | Care Quality Commission |
| Jan MacDonald | Group Manager Access and Information for Medicines and Standards, MHRA |
| Sumithra Maheswaran | Trust Pharmacist, London Ambulance Service NHS Trust |
| David Marshall | Health Improvement Adviser – Pharmacy, Care Inspectorate |
| Joela Matthews | Lead Pharmacist – Neurosciences, Barts Health NHS Trust; Neuroscience Group Committee Member, United Kingdom Clinical Pharmacy Association |
| Ewan Maule | Chair of Practice, Guild of Healthcare Pharmacists |
| Anne Melrose | Pharmacist Specialist, Care Quality Commission |
| Olivia Moswela | Lead Directorate Specialist Pharmacist, Neurosciences, Oxford University Hospitals NHS Trust |
| Joy Nicholson | Clinical Lead – Medicines and Pharmacy Team, Healthcare Improvement Scotland |
| Sue Oakley | Pharmaceutical Advisor, South Western Ambulance Service NHS Foundation Trust |
| Ngozi Onyele | Pharmacist Specialist, Care Quality Commission |
| Sandra Pryme | Training and Development Coordinator, Lancashire Teaching Hospitals NHS Foundation Trust; Representative of the Association for Perioperative Practice |
| Martin Pratt | Pharmacy Director, Gloucestershire Hospitals NHS Foundation Trust |
| Sue Renn | NHS Pharmaceutical Aseptic Services Group |
| Paula Russell | Former North East Ambulance Pharmacy Advisor, North East Ambulance Service Foundation Trust |
| Helen Sammons | Consultant Paediatrician, Chair of the Royal College of Paediatrics and Child Health Medicines Committee |
| Stuart Sanders | Private GP, The Independent Doctors Federation |
| Julia Scott | Deputy Chief Pharmacist, Dartford and Gravesham NHS Trust |
| Catherine Smith | Service Development Pharmacist, Primary Care Leads Group |
| Fiona Smith | Professional Lead for Children and Young People’s Nursing, Royal College of Nursing |
| Alan Timmins | Lead Clinical Pharmacist – Acute, NHS Fife |
| Stephen Tomlin | Neonatal and Paediatric Pharmacists Group |
| Judith Vincent | Clinical Director for Pharmacy and Medicines Management, Abertawe Bro Morgannwg University Health Board |
| Nicola Wake | Lead Clinical Pharmacist – Safety and Governance, Northumbria Healthcare NHS Foundation Trust |
| Lisa Wall-Hayes | Medicines Management Lead, John Taylor Hospice |
| Nigel Westwood | Patient/Lay Member |
| Sharon White | Chief Executive Officer, School and Public Health Nurses Association |
| Sandra Wolper | Associate Director – Medicines Use and Safety, NHS Specialist Pharmacy Services |
RPS Team
| Sonia Garner | Lead Author, Professional Standards Advisor |
| Katie Perkins | Lead Author, Professional Support Pharmacist (to October 2017) |
| Catherine Picton | Chair of the Advisory Steering Group, Consultant to RPS |
| Rakhee Amin | Senior Professional Standards Pharmacist |
| Rebecca Braybrooks | Professional Support Administrator |
| Rachel Quinlan | Professional Support Pharmacist |
| Wing Tang | Head of Professional Standards |
Consultation respondents
We would like to thank all the individuals and organisations who sent in comments on the draft guidance. In all, 83 individuals and organisations responded to the consultation making over 1,600 individual comments.
Organisations
- Aintree University Hospital NHS Foundation Trust
- Association of Anaesthetists of Great Britain and Ireland
- Association of Pharmacy Technicians UK
- Barts Health NHS Trust
- Betsi Cadwaladr University Health Board
- Care Quality Commission
- Centre for Medication Safety and Service Quality
- Chief Pharmacists across London
- City Health Care Partnership Community Interest Company
- Community Pharmacy Patient Safety Group
- Controlled Drug Accountable Officer Scotland
- Dartford and Gravesham NHS Trust
- Doncaster and Bassetlaw NHS Trust
- European Board of Anaesthesiology
- GTD Healthcare
- Guild of Healthcare Pharmacists
- Harrogate and Rural District Clinical Commissioning Group
- Healthcare Improvement Scotland
- Hywel Dda University Health Board
- Imperial College Healthcare NHS Trust and UCL School of Pharmacy
- Lancashire Teaching Hospitals
- Leeds Clinical Commissioning Group Partnership
- Llanfrechfa Grange Hospital
- Manchester Foundation NHS Trust
- Manchester University NHS Foundation Trust
- Marie Stopes UK
- Medicines and Healthcare products Regulatory Agency
- NHS Fife Safe Use of Medicines Group
- NHS Greater Glasgow and Clyde
- NHS Improvement
- NHS Lanarkshire
- NHS Pharmaceutical Aseptic Services Group
- NHS Pharmaceutical Quality Assurance Committee
- NHS Specialist Pharmacy Service – Medicines Use and Safety
- North West NHS Hospital Trusts
- Northumbria Healthcare NHS Foundation Trust
- Nottinghamshire Healthcare NHS Foundation Trust
- Nottinghamshire Healthcare NHS Foundation Trust Offender Health
- Nursing and Midwifery Board
- Nursing and Midwifery Council
- Pharmacy Eastern Network
- Rowlands Pharmacy
- Royal College of Anaesthetists
- Royal College of Midwives
- Royal College of Nursing
- Sheffield Children’s NHS Foundation Trust
- Sheffield Health and Social Care NHS Foundation Trust
- Society and College of Radiographers
- Somerset Partnership NHS Foundation Trust
- South West London and St George’s Mental Health Trust
- Tees, Esk and Wear Valleys NHS Foundation Trust
- Warrington Clinical Commissioning Group
- Welsh Pharmaceutical Committee
- West Herts Hospitals NHS Trust
Individuals
- Iben Altman
- Sam Bateman
- Rachael Daniels
- Melanie Dowden
- Tracy Hall
- Karen Harrowing
- Gareth Holyfield
- Helen Huck
- Fran Husson
- Janette Knight
- Alice Lo
- Louise Maunick
- Lyn Middleton
- Ruth Miller
- Julie Moore
- Caroline Nathan
- Andy Norris
- Shelly Palmer
- Sumara Parvez
- William Rea
- Adrian Robertson
- Marion Russell
- Geraldine Smith
- Rob Sneyd
- Kam Takhar
- Lisa Wall-Hayes
- Hadar Zaman
Supporting resources
A range of resources to support the implementation of the Professional Guidance on the Safe and Secure Handling of Medicines have been developed following discussion of barriers to implementation during the public consultation process.
We’d love to hear from you if you have any case studies to share or any other suggestions to help implement these guidelines. Contact [email protected].
Professional guidance on the administration of medicines in healthcare settings
Co-produced with the Royal College of Nursing, this document provides principles-based guidance to ensure the safe administration of medicines by healthcare professionals.
Download here.
The RCN and RPS have issued a joint statement to support the implementation of statement 10 of the Professional guidance on the administration of medicines in healthcare settings. You can view the statement here.
Case studies
Sections
- Hospital case study: Ensuring safe storage of medicines at collection points
- Hospital case study: Risk assessment of a medical device used as a medicine
- Hospital case study: Room temperature monitoring – introduction of data loggers
- Hospital case study: Using a second thermometer to monitor fridge temperatures
- Primary care case study: Maintaining the cold chain
- Ambulance service case study: Distribution and cycling of paramedic drug packs
Hospital case study: Ensuring safe storage of medicines at collection points
The NHS Trust covers a rural population and because of the wide geography in the county people can find it difficult to access trust pharmacy to collect ongoing medicine supplies.In some circumstances it can be a long distance – up to 3 hours round trip or more and this can cause disruption in continuity of care which is critical when treating mental health issues.
The hospital pharmacy therefore, often received requests to collect medicines from another, more convenient, location.
As a result, the pharmacy undertook a detailed risk assessment of potential collection points to see whether they could ensure the receipt, storage and collection of these medicines followed safe and secure handling processes.
Based on the risk assessment, the pharmacy team developed a standard operating procedure (SOP) defining accountabilities and responsibilities along with the procedure to be followed and the records to be kept in each individual collection point/setting.
The procedure ensures that all medicine supplies are recorded on receipt, stored appropriately, and that they are able to identify when medicines have been collected and perhaps more importantly, when they haven’t been collected within the specified time frame.
There are a number of collection sites involved in the scheme including a community team base, a community hospital and several GP surgeries all allowing people to collect their medicines locally.
Relevant sections of SSHM include: 3.4, 3.11, 3.15, 3.38-3.40, 3.44, 3.48, 3.51.
Hospital case study: Medical device – risk assessing its use as a medicine
Juvéderm® is a range of CE-marked pre-filled syringes containing lidocaine 0.3% and hyaluronic acid, marketed for injection into the mid to deep dermis for correction of moderate to severe facial wrinkles and folds, or the lips for augmentation and correction of perioral rhytids. Hyaluronic acid acts as a filler, with lidocaine for pain relief.
Although classed as a medical device it was identified that an ENT consultant within the hospital was purchasing and using Juvéderm® for medical purposes – for injection into the vocal cords for the treatment of vocal cord paralysis.
The Medicines Management Committee in the Trust had not been consulted about the use of the product in this way and no risk assessments carried out.
The consultant was asked to complete a retrospective application for the product for submission to the Medicines Management Committee. This was because Juvéderm® contains lidocaine, which has the potential for harm if injected intravascularly, and the product is part of a range of products with the same name so there is potential for the wrong product to be ordered/administered.
The Medicines Management Team reviewed the evidence from retrospective studies and a small randomised controlled trial, which demonstrated that injection laryngoplasty for vocal cord disorders did indeed improve phonatory function of the larynx and quality of the voice.
In addition, a ‘Purchasing for Safety Risk Assessment’ was completed, which identified that a range of Juvéderm® products was available with different concentrations of hyaluronic acid, different volumes, and with/without lidocaine. In addition, the generic name does not follow the brand name on the packaging. There is no SPC or PIL, but manufacturer’s ‘Directions for Use’.
The clinical evidence justified the continued use of the product, however, it was recommended that the ordering, prescribing and administration should be by Head and Neck Consultants only, to ensure correct concentration of hyaluronic acid, as well as the appropriate volume are injected into the vocal cord(s). It was agreed that the product would continue to be purchased through the central purchasing system, i.e. not by pharmacy. The consultant was asked to liaise with the Trust Medical Device Coordinator to set up a system to be able to respond to any relevant medical device alerts or recalls. A mechanism to avoid diversion of this product was required to be put in place, and a patient information leaflet developed, which could also explain that the product was being used for a different purpose to that which the manufacturer intends.
Relevant sections of SSHM include: 1.3, 2.8, 2.15, 2.21, 3.6, 3.8, 3.10.
Hospital case study: Room temperature monitoring – introduction of data loggers
Product licence storage specifications require that most medicines are stored below 25°C. However, there are many occasions when this is difficult to control such as during an occasional heatwave or in the winter when all the radiators are turned on.
During the summer, temperatures over 30°C were recorded in a clinic but there was no clear action plan for the staff to follow. Did all the medicines need to be discarded? Did expiry dates need reducing?
After much investigation the following were initiated:
- Data loggers were purchased for each locality. These data loggers are programmed with software that works out the mean kinetic temperature (MKT). MKT gives the average temperature that the medicines have been exposed to in a 24 hour period.
- When a team record a temperature above 25°C they take steps to reduce the temperature and monitor every day that week. If at the end of the week the temperatures are still high the pharmacy are contacted and a data logger requested.
- Using a data logger means that more accurate information can be provided, rather than relying on a maximum reading.
- In this instance, the clinic that had recorded temperatures above 30°C were informed that the MKT reading was below 25°C so on average their medicines were not being stored outside of parameters. This prevented the need to destroy medicines or reduce expiry dates.
What this has meant in practice:
Having a robust system in place with a detailed procedure has helped support staff to feel confident in the safe storage of their medicines.
Relevant sections of SSHM include: 3.39, 3.56, A23-24, A29.
Hospital based case study: Using a second thermometer to monitor fridge temperatures – ensuring the integrity of vaccines stored in the fridge
Although the vaccine fridge had an inbuilt digital temperature display that was checked and recorded daily, the pharmacy team believed the fridge felt exceptionally cold even though the temperature recorded was always between the required +2°C to +8°C.To test this, a cup of water was placed inside and after one hour the team reported that the water had frozen.
As a check, a second (external) digital thermometer was placed inside and the temperature recorded was 0°C.
An engineer confirmed that the inbuilt display was faulty and therefore the team had unknowingly been recording incorrect temperatures. Several thousand pounds worth of vaccines were compromised and therefore, all vaccines were destroyed. Freezing temperatures can make the vaccines inactive and unusable; it can also cause hairline cracks in glass containers or cause split seams in plastic ampoules which can facilitate bacterial contamination.
To prevent this happening again, the following action was taken:
- All fridges were issued with a second (external) digital thermometer to provide assurance that the inbuilt was working correctly.
- Temperature monitoring sheets were adapted to include two recordings daily (internal and external thermometer).
- If displays were faulty these were replaced – in some cases the fridges were condemned.
An unforeseen benefit is that the second thermometer, being independent of the main electricity supply, provides information in the event of a power failure. This ensures compliance with ‘Immunisation against infectious disease’ (also known as ‘The Green Book’) published by Public Health England.
Since the introduction of the second thermometer the pharmacy team has been alerted to temperature issues sooner than they would have been previously which has meant fewer vaccines have had to be destroyed and patient safety can be assured.
Relevant sections of SSHM include: 3.39, 3.56, A23-A33.
Primary care based case study: Maintaining the cold chain – ensuring the efficient storage of fridge lines in a GP practice
By chance one of the GPs at a practice found two vaccine deliveries behind the main reception area. Both of these deliveries contained fridge lines. One delivery had been out of the fridge for about one hour; the other package had been out of the fridge for at least six days and was warm to touch.
Both packages were marked ‘not for use’ and refrigerated pending investigation and risk assessment of the individual products.(NB: The pack which was out of the fridge for six hours had to be destroyed.)
Several measures were subsequently put in place or reinforced to prevent this from occurring again:
- All deliveries requiring refrigerated storage are clearly marked as ‘fridge’
- The delivery staff alert reception staff when a fridge item is included
- Reception staff are aware of the need to refrigerate these items promptly and that the items should be given to nurses to put in the fridge, or in their absence, put in immediately
- All new staff are now trained during their induction on the importance of maintaining the cold chain and regular update training sessions are held for existing staff.
An incidental finding was that there was no dedicated area for the dispensary deliveries to be stored on receipt. The reception team suggested a ‘blue box’ storage scheme whereby all (non-fridge line) medicines packages received are placed in a blue box.
This blue box idea has worked well as an intervention generally keeping handed-in medicines, dressings waiting for the practice nurse, travel drugs waiting to be picked up, implants delivered from the local pharmacy etc, in a more secure holding area rather than floating around in reception.
Relevant sections of SSHM include: 3.14, 3.44, 3.52, 3.56, A23.
Ambulance service case study – Distribution and cycling of paramedic drug packs
Maintaining a safe, secure and consistent supply of medicines across a geographically dispersed mobile workforce is a considerable challenge.
In order to achieve this, the ambulance service trust utilises a system of sealed bar-coded paramedic drugs packs with tamper evident seals packed and delivered by a dedicated team. Paramedic drugs bags are packed using a standardised layout before being sealed and stamped with an expiry date. Each bag is issued with a unique alphanumeric code which is then scanned and entered into a bespoke app via electronic tablets situated in medicines management areas at individual ambulance stations.
When equipping vehicles at the start of an operational shift, paramedics scan out the required drugs packs using the same app. At the end of the shift the bag is re-scanned using the app and designated as used or unused. Unused or out of date bags are then collected and returned for replenishment and redistribution.
The system provides real time data relating to pack location and drugs usage, enabling tracking and audit and facilitating recall of medicines if required.
Relevant sections of SSHM include: 3.11, 3.12, 3.21.
FAQs
Does this guidance replace the Nursing and Midwifery Council Medicines Management Standards?
No. This is a revision of an existing document.
The guidance can however, be used by nurses and midwives to support the safe and secure handling of medicines but it is not a direct replacement for the NMC standards.
Does this guidance cover community pharmacy? (Section 2.5)
Yes. The core principles and the framework for the safe and secure handling of medicines apply across all areas of practice. However not every stage of the framework will be applicable in every setting.
Does this guidance cover independent clinics such as aesthetic clinics or slimming clinic? (Section 2.5)
Yes. The core principles and the framework for the safe and secure handling of medicines apply across all areas of practice including aesthetic clinics and slimming clinics.
However not every stage of the framework will be applicable in every setting.
Does the guidance cover people in their own home? (Section 2.6)
No. Medicines that are obtained and stored by people in their own homes are not covered by this document; however, some of the principles are likely to apply and be of use to health and care professionals who work in peoples’ homes.
Feedback
If you have any comments on this guidance or suggestions as to how the guidance can be further developed please contact the Professional Support team at [email protected].
References
- National Pharmacy Clinical Trials Advisory Group. (2013). Professional Guidance on Pharmacy Services for Clinical Trials. (under review)
- Royal Pharmaceutical Society and NHS Pharmaceutical Quality Assurance Committee. (2016). Standards for Quality Assurance of Aseptic Preparation Services.
- See also: Royal Pharmaceutical Society. (2013). Medicines Optimisation: Helping patients to make the most of medicines. Good practice guidance for healthcare professionals in England.
- National Institute for health and Care Excellence. (2014). Social care guideline SC1: Managing medicines in care homes.
- National Institute for health and Care Excellence. (2017). NICE guideline 67: Managing medicines for adults receiving social care in the community.
- General Pharmaceutical Council. (2017). Standards for pharmacy professionals.
- Nursing and Midwifery Council. (2018). The Code: Professional standards of practice and behaviour for nurses and midwives and nursing associates.
- Nursing and Midwifery Council. Delegation and accountability. (Accessed 28.06.18)
- Health and Care Professions Council. (2016). Standards of conduct, performance and ethics.
- General Medical Council. (2013). Good medical practice.
- General Dental Council. (2013). Standards for the Dental Team.
- Department of Health. (2013) Health Building Note 14-01: Pharmacy and radiopharmacy facilities.
- General Pharmaceutical Council. (2018). Standards for registered pharmacies.
- International Organization for Standardization. (2015) ISO 9001 Quality Management.
- Royal Pharmaceutical Society. The right culture: quick reference guide. (Accessed 15.08.18)
- NHS Improvement. (2018). A just culture.
- Royal Pharmaceutical Society. (2016). Professional standards for the reporting, learning, sharing, taking action and review of incidents.
- Pharmacy QS. Quality Systems for Pharmacy. (Accessed 17.01.18)
- Royal Pharmaceutical Society. (2011). Keeping patients safe when they transfer between care providers – getting the medicines right.
- NHS England. (2014) Patient safety alert: Risks arising from breakdown and failure to act on communication during handover at the time of discharge from secondary care.
- European Commission. Falsified Medicines Directive. (Accessed 24.05.18)
- NHS England. (2018). Standing Financial Instructions.
- Specialist Pharmacy Service. (2018). Best Practice Standards for managing medicines shortages in NHS hospitals.
- Royal Pharmaceutical Society. (2015). Professional Guidance for the Procurement and Supply of Specials.
- General Pharmaceutical Council. (2017) In Practice: Guidance on Consent.
- General Medical Council. (2008). Consent: Patients and Doctors Making Decisions Together.
- Care Quality Commission. Guidance for providers. Health and Social Care Act 2008 (Regulated Activities) Regulations 2014: Regulation 11: Need for consent. (Accessed 31.01.18)
- Nursing and Midwifery Council. (2018). The Code: Professional standards of practice and behaviour for nurses and midwives and nursing associates.
- Mental Capacity Act 2005. (Accessed 31.01.18)
- Office of the Public Guardian. (2013) Mental Capacity Act Code of Practice.
- National Data Guardian. (Accessed 31.01.18)
- Adults with Incapacity (Scotland) Act 2000. (Accessed 31.01.18)
- Adults with Incapacity (Scotland) Act 2000 – Codes of Practice. (Accessed 31.01.18)
- Royal College of Nursing. (2017) Principles of Consent – guidance for nursing staff.
- Specialist Pharmacy Service. (2017). To PGD or not to PGD that is the question.
- Medicines and Healthcare products Regulatory Agency. (2004) Rules for the sale, supply and administration of medicines for specific healthcare professionals.
- British National Formulary. Emergency supply of medicines. (Accessed 23.05.18)
- Specialist Pharmacy Service. (2018). Questions about Patient Specific Directions (PSD).
- British National Formulary. Emergency supply of medicines. (Accessed 23.05.18)
- Specialist Pharmacy Service. Medicines Matters: A guide to mechanisms for the prescribing, supply and administration of medicines (in England).
- Royal Pharmaceutical Society. (2018) Medicines, Ethics and Practice – the Professional Guide for Pharmacists.
- Specialist Pharmacy Service. (2014). What are the legal requirements for labelling a Prescription Only Medicine (POM) issued via a PGD before supply to the patient?
- Specialist Pharmacy Service. (2011). Questions about labelling and dose specification in PGD for P and GSL medicines.
- Medicines and Healthcare products Regulatory Agency. (2014). Medicines: packaging, labelling and patient information leaflets.
- Medicines and Healthcare products Regulatory Agency. (2014). Best practice in the labelling and packaging of medicines.
- Royal Pharmaceutical Society and NHS Pharmaceutical Quality Assurance Committee. (2016). Quality Assurance of Aseptic Preparation Services: Standards.
- UK Radiopharmacy Group. (2017). Responsibilities of Chief Pharmacists for the purchase, receipt, storage, supply and disposal of radiopharmaceuticals.
- World Health Organisation. WHO Guidelines on Good Manufacturing Practices for radiopharmaceutical products. (Accessed 15.08/18)
- National Patient Safety Agency. (2007). NPSA Alert – Promoting safer use of injectable medicines.
- National Patient Safety Agency. Safe Anaesthesia Liaison Group. (2012). Patient Safety Update including the summary of reported incidents relating to anaesthesia 1 January 2012 to 30 March 2012.
- Royal College of Nursing. (2016). Standards for infusion therapy.
- Specialist Pharmacy Service. (2018). Archived Patient (Medication) Safety Alerts from the NPSA and SPS resources to support their implementation.
- Specialist Pharmacy Service. (2018). Archived NPSA Signals – Emerging issues from national review of serious patient safety incidents 2009-2012 and supporting SPS resources.
- NHS Scotland. (2002). Good Practice Statement for the Preparation of Injections in Near-Patient Areas, including Clinical and Home Environments.
- Department of Health. (2013). Health Technical Memorandum 07-01: Safe management of healthcare waste.
- Health Facilities Scotland. (2015). NHS Scotland Waste Management Guidance.
- National Institute for health and Care Excellence. (2016). NICE guideline 46: Controlled drugs: safe use and management.
- Specialist Pharmacy Service. (2012). Principles on the Disposal of Waste Pharmaceuticals used within Community Health Services.
- Advisory Committee on the Misuse of Drugs. (2016). ACMD report on diversion and illicit supply of medicines.
- Health Protection Scotland. (2017). Guidance on vaccine storage and handling.
- National Institute for health and Care Excellence. (2016). NICE guideline 46: Controlled drugs: safe use and management.
- Home Office. (2016). Guidance for the safe custody of controlled drugs and drug precursors in transit.
- Department for Transport. (2016). Commercial and private carriage of oxygen cylinders by road.
- Health and Safety Executive. Carriage of dangerous goods. (Accessed 15.08.18)
- UK Radiopharmacy Group. (2017). Responsibilities of Chief Pharmacists for the purchase and supply of radiopharmaceuticals.
- Department of Health. Collection: DH building notes. (Accessed 23.05.18)
- Home Office. (2016). Security guidance for all existing or prospective Home Office Controlled Drug Licensees and/or Precursor Chemical Licensees or Registrants.
- NHS. (2016). The use of vaccines that have been temporarily stored outside the recommended temperature range.
- Home Office. (2016). Security guidance for all existing or prospective Home Office Controlled Drug Licensees and/or Precursor Chemical Licensees or Registrants.
- Medicines and Healthcare products Regulatory Agency. Drug-name confusion: reminder to be vigilant for potential errors. (Accessed 29.10.18)
- NHS Improvement. Patient Safety Alerts. (Accessed 08.11.18)
- Specialist Pharmacy Service. (2018). Archived Patient (Medication) Safety Alerts from the NPSA and SPS resources to support their implementation.
- Department of Health. (2006). NHS estates guidance for medical gas pipeline systems (HTM 02-01).
- British Thoracic Society Emergency Oxygen Guideline Development Group. (2017). Thorax. BTS Guideline for Oxygen Use in Adults in Healthcare and Emergency Settings.
- British Compressed Gases Association. (2016). Code of Practice 44. The Storage of Gas Cylinders.
- NHS Wales. (2016). Patient Safety Notice PSN 030. The safe storage of medicines: Cupboards.
- Resuscitation Council (UK). (2016). Keeping Resuscitation Drugs Locked Away.
- NHS. (2016). The use of vaccines that have been temporarily stored outside the recommended temperature range.
- NHS Pharmaceutical Quality Assurance Committee. (2015). Risk Management of Medicines in Clinical Areas: Temperature Control.
- Department of Health. (2013). Immunisation Against Infection Disease – ‘The Green Book’.
- Medicines and Healthcare products Regulatory Agency. (2017). Rules and Guidance for Pharmaceutical Distributors.
- Welsh Government and NHS Wales. (2015). Patient Safety Notice PSN 015: Storage of Medicines: Refrigerators.
- Home Office, Security guidance for all existing or prospective Home Office Controlled Drug Licensees and/or Precursor Chemical Licensees or Registrants. 2016.
- National Patient Safety Agency. Safer practice notice: Ensuring safer practice with high dose ampoules of diamorphine and morphine. 2006.
- National Patient Safety Agency. Safe Anaesthesia Liaison Group. (2012). Patient Safety Update including the summary of reported incidents relating to anaesthesia 1 January 2012 to 30 March 2012.
- National Patient Safety Agency. (2007). NPSA Alert – Promoting safer use of injectable medicines.
- Royal College of Nursing. (2016). Standards for infusion therapy.
- Department of Health. (2013). Immunisation Against Infection Disease – ‘The Green Book’.
- Royal College of Anaesthetists. (2018). Guidelines for the Provision of Anaesthesia Services for Intra-operative care.
- National Patient Safety Agency. (2007). Patient Safety Alert: Safer practice with epidural injections and infusions.
- Royal College of Anaesthetists. Can an Operating Department Practitioner, Anaesthetic Nurse or Physicians’ Assistant (Anaesthesia) draw up drugs for the anaesthetist in the operating theatre? (Accessed 01.02.18)
- College of Operating Department Practitioners. (2009). Scope of Practice.
- NHS Improvement. (2016). Patient Safety Alert: Restricted use of open systems for injectable medication.
- NHS England. (2015). Patient Safety Alert: Risk of death or severe harm due to inadvertent injection of skin preparation solution.
- British Society for Interventional Radiology. (2016). Advice – Risk of death or severe harm due to inadvertent injection.
- Royal College of Anaesthetists. (2017). Guidance on the provision of anaesthesia services for acute pain services.
- NHS Improvement. (2017). Patient Safety Alert: Resources to support safe transition from the Luer connector to NRFit for intrathecal and epidural procedures, and delivery of regional blocks.
- Association of Anaesthetists of Great Britain and Ireland. (2014). Arterial line blood sampling: preventing hypoglycaemic brain injury.
- NHS Improvement. (2018). Patient Safety Alert: Risk of death or severe harm from inadvertent intravenous administration of solid organ perfusion fluids.